Are you using ropi for spinals? Is that off label use?
Are you using ropi for spinals? Is that off label use?


pubmed.ncbi.nlm.nih.gov/10551572/ pubmed.ncbi.nlm.nih.gov/9728842/ pmc.ncbi.nlm.nih.gov/articles/PMC... pubmed.ncbi.nlm.nih.gov/11878524/ pubmed.ncbi.nlm.nih.gov/38435645/ pubmed.ncbi.nlm.nih.gov/27106206/ pmc.ncbi.nlm.nih.gov/articles/PMC... pubmed.ncbi.nlm.nih.gov/29192639/
I’m sure it’s fine…but still off-label. And here that means documented informed consent for each patient
Ugh that's a drag
It's licensed in most european countries though...
no it is not.
For example: Germany (direct link to Bfarm.de is not working), Austria (aspregister.basg.gv.at/document/ser...), Switzerland (compendium.ch/product/1169...), Netherlands (www.geneesmiddeleninformatiebank.nl/smpc/h27204_...)
Ha, Thanks! I stand partially corrected. (depends on sources)
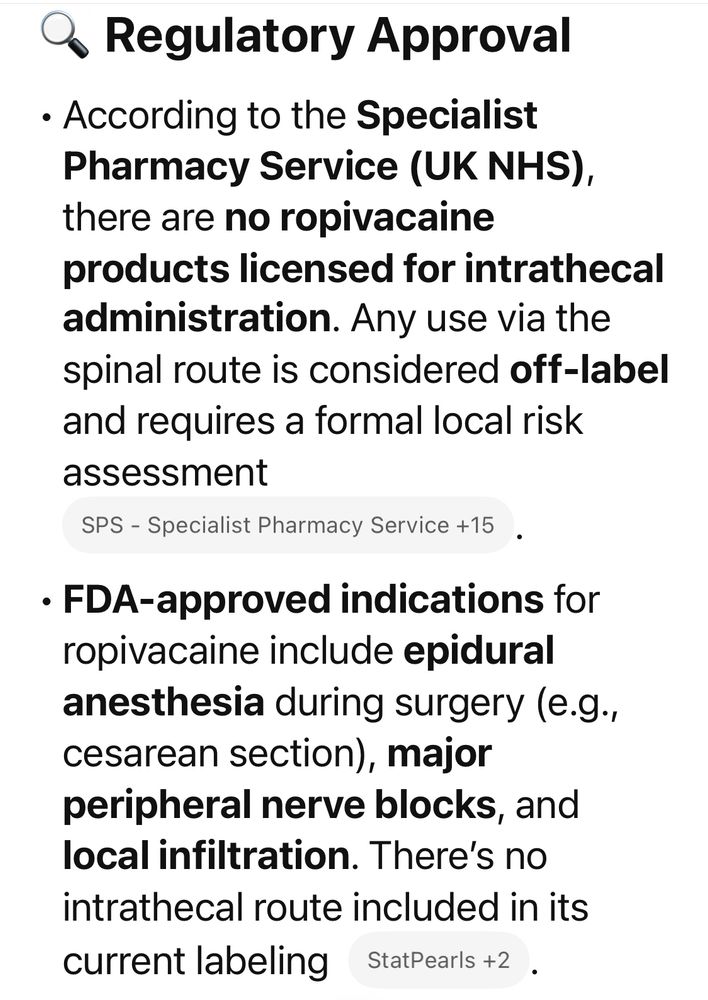
I'll quote your source back at you then 😉 This is ChatGPTs answer in english

😁👍🏼
Not for intrathecal use
I've been doing ropi/fent spinals for caesars for about 20 years. Main advantages are that it's extremely fast and if you get significant hypotension you can tip the pt into trendellenberg without making things worse. Our local audit showed it also causes less urinary retention.
interesting! How much of both do you give?
15mg Rop which works out to be either 1.5mL of 1% Rop or 2mL of 0.75%, together with 0.3mL Fent (15mcg) +/- 0.5mL Morphine (100mcg). Total injectate 2.3 or 2.8mL depending on whether you add the morphine. I sometimes add 0.1-0.3mL Ropi depending on the height of the pt.
sounds excellent! unfortunately Ropi intrathecal here is a no. Also we don’t have dilute morphine (ours is 5mg/ml) so potential big error.
Colleagues thought I was strange (which Ι am) until a few years ago when there was a local scare about the availability of heavy marcain. They then accepted it as a valid alternative and some have since joined me in making it their routine technique.
It does require more attention and good communication/coordination - it works very fast and if the team don't get the pt horizontal reasonably promptly you can get a high spinal. In ~50% of pts in the time it takes to get from removing the needle to getting the pt flat the block is already at T6.

I wonder why it’s a quicker onset. I always understood ropiv and bupiv to have similar onset for regional blocks
Heavy bupiv that is traditionally used takes time to diffuse. I suspect if you use plain bupiv the onset times are similar. With ropiv there is a tendency for the sensory block to exceed the motor block by a couple of levels.
During my training we uses bupivacaine 0.5% plain for csections with similar effect
Yes - I would say that the differential motor/sensory block you get with ropivicaine is more forgiving for C-section.